Kidney Masses
The incidental discovery of a mass on the kidney has become a commonplace occurrence now that imaging modalities such as ultrasound, MRI and particularly CT scanning is so prevalent. It is of course very scary to be told that by accident a mass or lesion has been found on one’s kidney, and almost always in such a circumstance a patient will be referred for counseling or perhaps even surgery to remove the mass. It is important to remember however that many masses or suspicious lesions may not need to be removed, may not be cancerous, and even if cancerous are usually cured with removal alone.
Kidney cysts can be very normal findings, and if they have no suspicious characteristics may not require further treatment or even to be followed.
During a consultation, where a patient must bring his/her actual scan on disc for review by us, the first thing to determine are the characteristics and appearance of the kidney lesion. Kidney cysts can be very normal findings, and if they have no suspicious characteristics may not require further treatment or even to be followed. Such cysts are called “simple” cysts and are usually definitively diagnosed with ultrasound or a CT scan with IV contrast.

However, some cysts can be classified as “complex”, and such cysts do carry some risk of malignancy. A CT scan with IV contrast is mandatory if at all possible in such circumstances so that the Urologist can assign a “Bosniak score”. This scoring system uses specific characteristics of the cyst like wall thickness, internal septations, calcifications and whether the cyst “enhances” to generate a score that predicts malignancy risk. A Bosniak 1 cyst is a simple cyst and would not be followed. A Bosniak 4 cyst is considered an enhancing renal mass and must be assumed to be malignant and thus treated accordingly. It is the intermediate grade complex cyst that requires judgment and counseling as to proper next steps. A Bosniak 2 cyst has a less than 1% chance of being malignant. They may or may not be followed based on the clinician’s judgment. A slightly more suspicious score is a Bosniak 2F, which will be malignant 5% of the time. These complex cysts are typically followed until complete stability is demonstrated over time. A Bosniak 3 cyst will be cancerous 50% of the time and unless there are co-morbidities that preclude surgery are usually dealt with in a similar fashion to solid renal/kidney masses.
If a kidney lesion is a solid mass, particularly one that picks up blood and thus “enhances” on contrast CT, it is considered malignant until proven otherwise. In the era of CT scan however, masses are found at a much smaller size than ever before. Now, if a mass is small, less than 2 cm, up to 20-25% of such lesions may be benign. The most common benign renal mass is called an oncocytoma. Oncocytomas have a typical appearance when large, but when small look similar to malignancy. Another common benign renal mass, more common in fertile women, is called an Angiomyolipoma. Such masses often contain fat that can be demonstrated on CT allowing for a definitive diagnosis by X-Ray alone. Angiomyolipomas are usually followed unless greater than 4 cm in largest dimension. Such lesions are usually treated with percutaneous embolization and not surgery.
Most patients will wonder why a biopsy is not routinely performed to differentiate between benign and malignant renal masses, and this is currently a controversial area in Urology. The classic thinking has been that nearly 90% of all enhancing renal masses are malignant. If a percutaneous biopsy is performed showing malignancy, it actually has not helped the management of a mass in that, as a default, surgery was to be performed anyway. If the biopsy is indeterminate, as it often is due to lack of providing a large amount of tissue for review to the Pathologist, one must still act on the assumption that cancer is present. If the tissue is read as benign, unfortunately this test has only an approximate 85% sensitivity, and thus cancer could have been missed. In all situations, a biopsy is a separate procedure with risks such as tumor spillage, bowel injury, hemorrhage and needle site seeding with cancer. Some centers feel that a biopsy can help grade cancer as high or low grade, thus making it easy to offer some patients with renal masses conservative management, but this has not become the standard. Thus, the decision to proceed with treatment is typically based on statistical likelihood and not an actual biopsy.
At Urologic Surgeons of Washington, most renal masses less than 2.5 cm are followed for a period of time and not automatically treated. This threshold is sometimes even higher if surgery would be unsafe for a certain patient.
There is strong justification in the literature that small renal masses, even ones that are suspicious for malignancy, can be followed and only removed if growing. Most kidney tumors grow very slowly, and if below a certain size threshold have a very low, less than 1%, risk of metastasizing or spreading. At Urologic Surgeons of Washington, most renal masses less than 2.5 cm are followed for a period of time and not automatically treated. This threshold is sometimes even higher if surgery would be unsafe for a certain patient.
However, if a suspicious mass or complex cyst is larger than 2.5cm, treatment is typically offered. Treatment for renal masses is predominately surgical. Radiation and/or chemotherapy play almost no role in the initial management of a kidney mass unless proof of metastasis exists. In certain cases, a patient may be a candidate for percutaneous management such as freezing the tumor (cryotherapy) or heating the tumor (microwave or ultrasound). Such a patient would be an elderly patient or a patient with co-morbidities precluding surgery, and a tumor location and size that is amenable to such an approach. Cryotherapy is sometimes offered laparascopically by Dr. Engel, but only in cases where laparoscopic partial nephrectomy is precluded due to the location of the tumor.
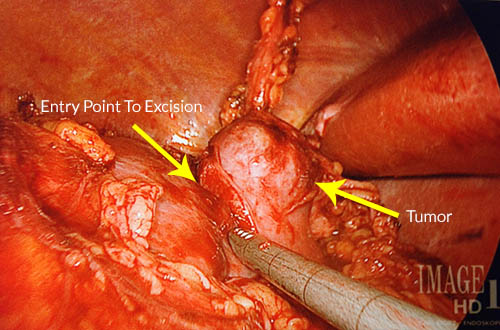
The contemporary mainstay of surgery for renal masses is laparoscopy, the act of performing abdominal surgery by inflating the abdomen with carbon dioxide, inserting a camera and several instruments that allow for surgery through small incisions with a rapid recovery. Once it is determined that treatment of a kidney mass is necessary, the next step is to review the actual films, usually a contrast CT, to determine if removing only the tumor is feasible. This is always the desired approach, and in Dr. Engel’s hands will always be attempted. In cases however where the tumor is in a central location, invades deeply into the center of the kidney, or if negative margins cannot be assured in the operating room, the entire kidney will be removed. One only needs one healthy kidney, so in such a circumstance the patient is not usually adversely affected.
There are several laparoscopic tools that Dr. Engel employs to perform laparoscopic kidney surgery. Robotic surgery is often used to dissect out the tumor from the kidney and perform reconstruction (Robotic partial nephrectomy). Hand-assisted laparoscopy is a style of laparoscopy where one hand is inside the abdomen and one hand outside. Dr. Engel performs hand-assisted laparoscopy when it is known ahead of time that the entire kidney is to be removed (Hand-assisted laparoscopic nephrectomy), or in high risk cases such as chronic kidney failure where it is desirable not to clamp the blood vessels to the kidney (Hand-assisted partial nephrectomy). Sometimes only standard laparoscopy is used such as for a very small kidney. The patient will consent to all approaches so that Dr. Engel is free to use whatever tools are required to fit the particular circumstance found at the time of surgery.
The most common cell type found in kidney cancer is called clear cell renal cell carcinoma, but variants such as papillary, sarcomatoid, medullary and others are seen. Transitional cell carcinoma (TCC) is not uncommon, is typically found in smokers, and arises from the lining of the kidney rather than the functioning kidney tissue itself. TCC of the renal pelvis is more similar to bladder cancer than kidney cancer, carries a higher metastasis risk, and if found, typically necessitates removal of not only the entire kidney but also the entire ureter as well. Thus, if TCC of the renal pelvis or collecting system is found, a patient is offer a “nephro-ureterectomy”, also performed laparoscopically by Dr. Engel.
The risks present for all laparoscopic kidney surgeries include of course pain, infection and bleeding. But, since we are in the abdomen when performing laparoscopy, there is always the risk of inadvertent bowel injury that will require repair. It is for this reason that all patients will undergo a full mechanical and antibiotic bowel prep. All patients will have to consent to a total nephrectomy based on the surgeon’s judgment, as well as conversion to an open procedure if necessary. Conversion to open has been extremely rare for Dr. Engel. Patients will stay typically 2 days (total nephrectomy) or 3 days (partial nephrectomy) in the hospital. In the case of partial nephrectomy, additional possible rare complications are urine leak or bleeding that may require further procedures to address. After discharge, the hallmark of proper recovery after laparoscopic kidney surgery is slow and steady improvement in how one feels. The bowels will take some days to be regular, but typically patients are back to work within 10 days to 2 week. A post-operative visit just before returning to work is scheduled to go over the pathology report.
Please feel free to view videos of Dr. Engel performing a Hand-Assisted Total Nephrectomy, a Robotic Partial Nephrectomy, and a Hand-Assisted Partial Nephrectomy (coming soon) from the Procedures section of this site.