Urethral Strictures
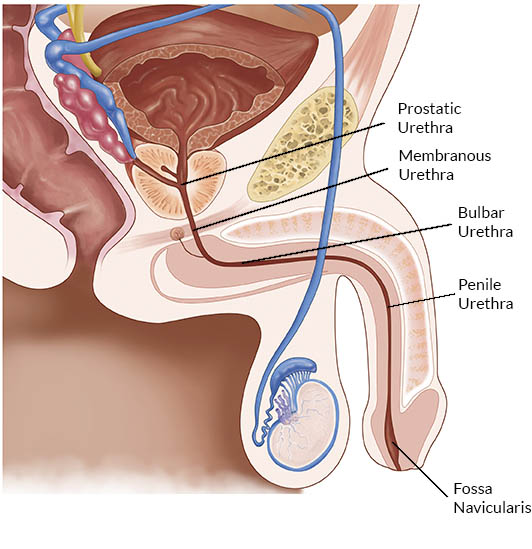 Another urologic condition we see and treat regularly is urethral strictures. The urethra is the tube that carries urine through the prostate and penis as shown in the diagram, and a stricture is essentially a scar that limits urine flow. The male urethra has several distinct anatomic segments, and it is valuable to go over them here briefly. Technically speaking, the urethra starts at the bladder base or neck and travels through the prostate as the prostatic urethra. The most common cause for prostatic urethral strictures would be previous radiation therapy for prostate cancer or previous operations for an enlarged prostate such as a TURP. Just beyond this point, in the area which includes the voluntary urinary sphincter, is the membranous urethra. This can also be narrowed or scarred by radiation therapy but is most commonly injured as a result of pelvic trauma or pelvic fracture. Repair of the membranous urethra is complicated, often resulting in incontinence, and will not be discussed further here.
Another urologic condition we see and treat regularly is urethral strictures. The urethra is the tube that carries urine through the prostate and penis as shown in the diagram, and a stricture is essentially a scar that limits urine flow. The male urethra has several distinct anatomic segments, and it is valuable to go over them here briefly. Technically speaking, the urethra starts at the bladder base or neck and travels through the prostate as the prostatic urethra. The most common cause for prostatic urethral strictures would be previous radiation therapy for prostate cancer or previous operations for an enlarged prostate such as a TURP. Just beyond this point, in the area which includes the voluntary urinary sphincter, is the membranous urethra. This can also be narrowed or scarred by radiation therapy but is most commonly injured as a result of pelvic trauma or pelvic fracture. Repair of the membranous urethra is complicated, often resulting in incontinence, and will not be discussed further here.
After the short membranous urethra comes what should be the widest portion of the male urethra called the bulbar urethra. Here is where the urethra changes course upwards to reach the penis. Men sit on their bulbar urethras, and it is this site that is most commonly strictured or scarred. Such patients are usually younger men and a distinct cause of the stricture is usually elusive. The most common causes would be trauma from falling on one’s crotch, being kicked, or previous STDs affecting the urethra such as chlamydia or gonorrhea. Previous surgery or instrumentation is another cause.
The length of the urethra that traverses most of the penis is called the penile urethra, or pendulous urethra, or sometimes the anterior urethra. Strictures here are less common and may be associated with inflammatory conditions of the glans such as balanitis xerotica obliterans or lichen sclerosis. These are tough strictures to treat, often requiring more complicated reconstructive procedures, and can be recurrent if an underlying disease is present.
Finally, the area of the urethra just under the glans (head of the penis), just before the meatus, is called the fossa navicularis. Strictures in this area are seen often after a catheter or scope has been placed in a man’s urethra, for instance after a TURP. These strictures often respond to simple dilation, and if recurrent can easily be managed by self-dilation. On rare occasions, reconstructive surgery is indicated.
Typically a patient with a urethral stricture will complain of a slow urinary stream, and a common telltale sign in a younger man is urinary dribbling after finishing at the toilet. A urinary infection may be what brings a stricture to light as well as episodes of blood in the urine. It is often a progressive problem, and when suspected the diagnosis is made by cystoscopy, or looking into the urethra with a scope in the office. If a stricture is found, often it will be investigated by an x-ray called a retrograde urethrogram to determine its exact location and length. Based on the findings, several treatment options can be employed.
The simplest treatment is dilation of the stricture. This is always performed with a fossa navicularis stricture due to its ease and effectiveness, or a membraneous stricture as this may be the only way to open the channel without causing incontinence. Otherwise, we employ dilation very sparingly because the recurrence rate after dilation is 80-90%, and each dilation can lengthen or worsen the stricture thus complicating its treatment. Our preferred approach for the initial presentation of a urethral stricture is to perform a minor procedure, under anesthesia, called a direct vision internal urethrotomy (DVIU). Here, the recurrence rate is still high at approximately 50% but is still far less than dilation and may be less traumatic to the urethra. The stricture is cut with a knife or laser using a scope.
Sometimes an injection of medicine (mitomycin-C or other) is made into the cut base of the stricture as well to try to decrease the recurrence rate. There are devices now in their initial stages of popularization that dilate the stricture and try to impregnate the stricture with these medicines as well, but superiority to a simple DVIU and injection has not at all been proven yet and they are very expensive. After the DVIU, a patient will typically wear a urinary catheter for a few days after a DVIU and should notice a dramatic improvement in their stream right away. Then, it is a function of being on the lookout for recurrence.
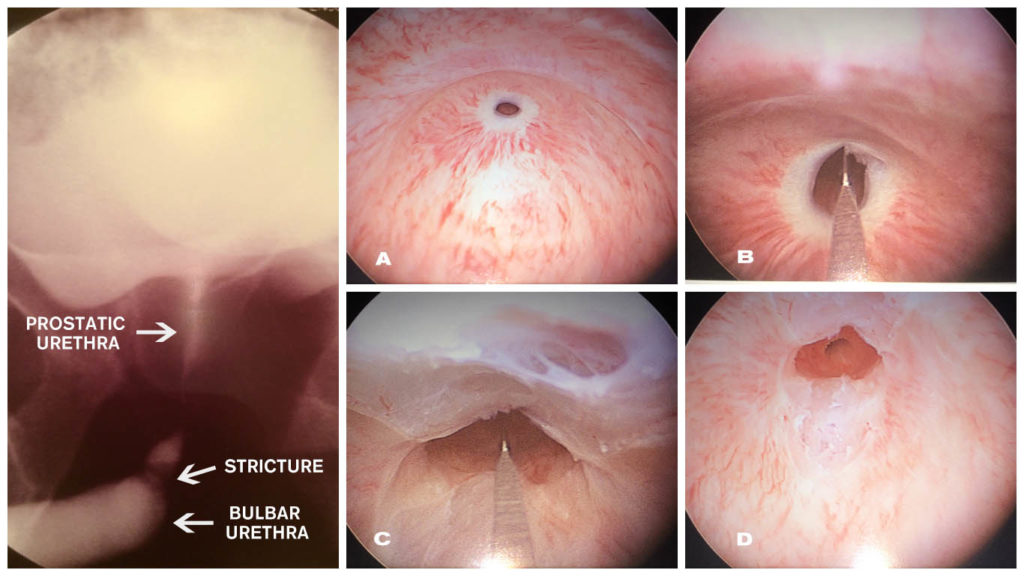
Internal Urethrotomy
A: Bulbar urethral stricture. B: Initial incision of stricture. C: Completion of incision.
D: Stricture now open, urinary sphincter shown.
If a stricture does recur, more aggressive solutions will be offered. A patient can always choose to undergo another DVIU, or even dilation, but at this point, such a patient must expect recurrence rates of over 90%, even with DVIU. If recurrence occurs after the first DVIU, Dr. Engel will offer a more permanent solution called a urethroplasty, a reconstructive procedure that Dr. Engel performs. A urethroplasty is a surgical repair of a stricture whereby the affected area is dissected and either fully excised with the good ends brought together with sutures (an anastomotic urethroplasty), or incised and the gap in the tubular urethra filled with tissue. Today, the preferred tissue to use is the lining of one’s cheek, called buccal mucosa. Over the years, many different tissue techniques have been used, including bladder mucosa, scrotal skin, foreskin, penile skin, and others. Buccal mucosa has largely replaced those tissues as the graft of choice and the introduction of its use greatly simplified and improved the treatment of recurrent urethral strictures.
For bulbar strictures less than 2cm, Dr. Engel will sometimes perform an anastomotic urethroplasty, whereas longer or anterior strictures will almost always call for a graft. With a buccal mucosa urethroplasty, the patient will have stitches inside the side of their mouth where the graft was taken which will dissolve over a few days. The feeling is similar to having bitten one’s cheek. The pain is not severe, and this site heals very rapidly. In addition, a catheter will have to stay in the urethra draining the bladder urine while the graft heals for 2-3 weeks. A urethroplasty is an outpatient procedure in Dr. Engel’s hands. Depending on the location and severity of the stricture a urethroplasty can afford a 93% success rate or better with no recurrence. Although this is more of an actual reconstructive surgery, with some mild recovery and the imposition of wearing a catheter strapped to one’s leg for a few weeks, the payoff of having this frustrating, recurrent problem removed from one’s life so that repeat lifelong procedures are avoided is invaluable and almost invariably makes a urethroplasty well worth undergoing in the long term.
Dr. Engel has been performing this type of surgery in the DC area for 25 years. He would be happy to see you if you suspect or have been diagnosed with a urethral stricture during an office consultation and offer the best approach for you.


